What is OCD?
When I ask most people about their understanding of Obsessive-Compulsive Disorder (OCD), they immediately picture someone who is highly organized, obsessed with cleaning and/or hand-washing, or someone who counts or checks the locks. While all of those descriptors encompass a small portion of symptoms that people with OCD experience, that list is not by any means exhaustive.
It is completely understandable why most people picture OCD to be this way- it is essentially the only way in which the media portrays it. And while the college students in my undergraduate classes may tease me for how often I reference TV shows and movies when discussing psychological phenomenon, the truth is that none of us are powerful enough to resist how media informs our cultural worldview. The biases created by this worldview can have major consequences. Case in point- there are many mental health professionals who will dismiss a potential diagnosis of OCD if the client does not report counting, checking, or washing behaviors.
But the truth is, OCD encompasses an incredibly diverse presentation of symptoms. So what truly is OCD?
The two categories of symptoms are embedded right in the name: obsessions and compulsions. An obsession refers to any intrusive thought, image, sensation, or idea that gets stuck in someone's head and causes significant distress. Like a catchy jingle, it feels impossible to shake this obsession loose. In an effort to relieve that increasing anxiety that this obsession causes, a client engages in some sort of compulsion. This compulsion refers to any behavior or thought that is used to "neutralize" the threat of the obsession. This can involve the aforementioned counting or checking, but also can involve harder-to-catch compulsions, like reassurance seeking (e.g., repeatedly asking if something is okay), mental rituals (i.e., mentally repeating a list over and over, or mentally reviewing a recent situation), avoidance, or subtly repeating an action until it feels "just right."
Therefore, all of these fictional patients meet a diagnosis for OCD:
Steve has a nagging thought that maybe he does not love his fiancée (obsession). To convince himself that he does love her, he forces himself to assess his level of attraction towards every person he sees on the street (mental compulsion).
Sally is terrified that she will accidentally hurt someone (obsession). To assuage her fear, she repeatedly asks her parents if she hurt them (reassurance compulsion). She also tries to avoid dangerous objects likes knives (avoidance compulsion).
Bobby keeps having the feeling that the sentences in his essay are not good or "right" enough (obsession). He re-writes sentences over and over, often not even changing a word, until that feeling goes away (repetition compulsion).
Jean is afraid she will forget to do her homework (obsession). She methodically and repeatedly reviews her homework list in her head until she feels better (mental compulsion).
Betty is very concerned about having an allergic reaction, even though she has never had one before (obsession). She avoids multiple major food groups that she believes may cause her to have a reaction (avoidance compulsion), and constantly asks her dad if foods are "safe" for her to eat (reassurance compulsion).
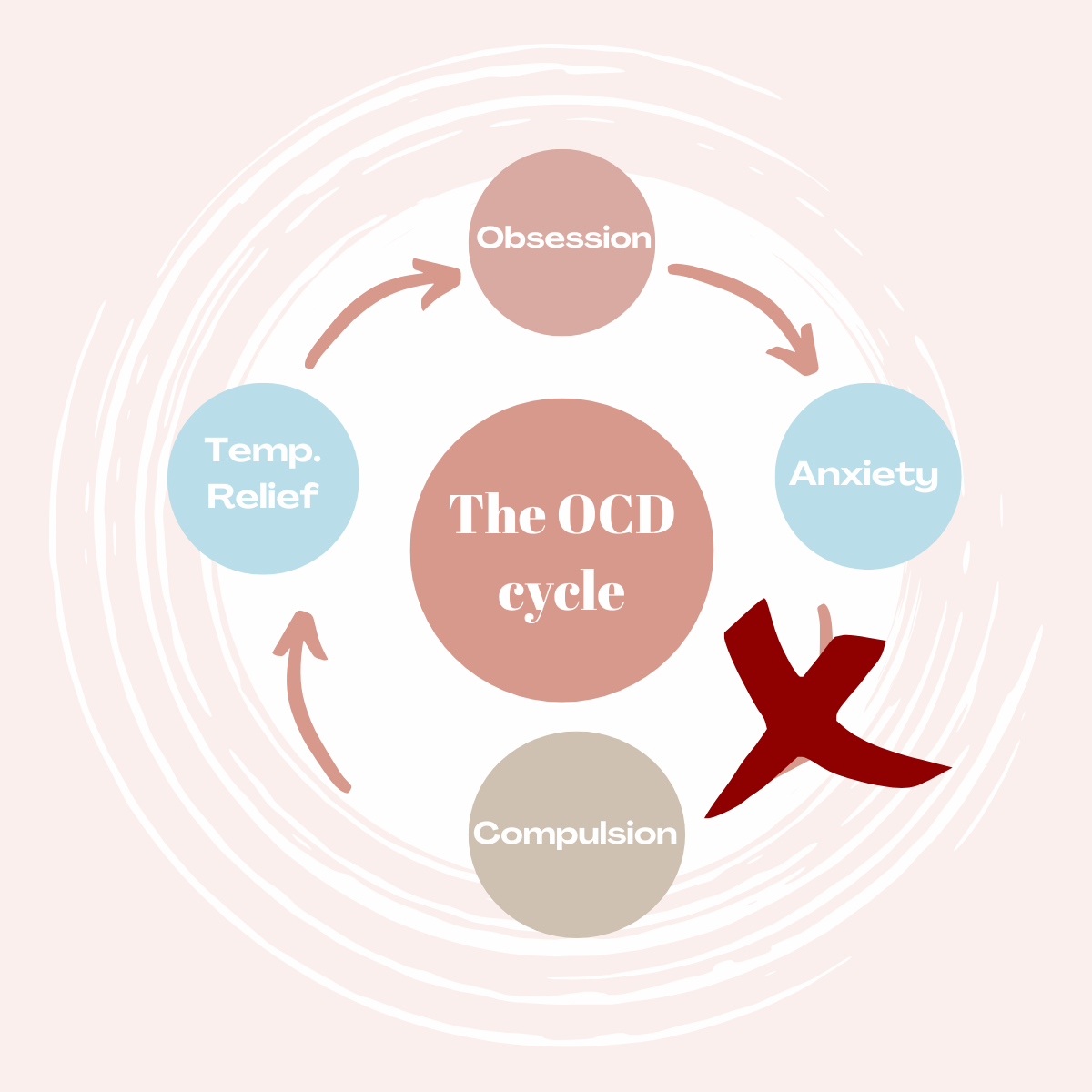
At first, the compulsion causes a reprieve from the anxiety causes by the obsession. But this reprieve is typically very brief, and soon the obsession begins once again. Because the brain has made the association between the compulsion and anxiety relief, the person will once again engage in the compulsion in an effort to find relief again. And so the cycle continues and deepens: obsession, anxiety, compulsion, temporary relief, and back again.

OCD is always either growing or shrinking, never staying stagnant. This means that, eventually, the compulsions will need to become "bigger" in order to provide the same level of relief. Steve may need to mentally review his potential attraction towards others several times; Sally may need to ask her mom more and more times if she has accidentally hurt her; Bobby may need to re-write his sentences more times; Jean may spend excessive time repeating her list; Betty may add more and more food groups to her "not safe" list. Eventually, the compulsion itself causes its own distress, but the cycle is so engrained at this point that it feels impossible to undo. At times, the cycle itself may even be unconscious.
So how is OCD treated? Many come into therapy hoping that the first step is to find a way to get rid of the obsessions and the anxiety that they cause. While this of course is the ultimate goal, treating OCD is different than treating a typical anxiety disorder. An intense discussion and exploration of the obsession- which would be common in therapy for non-OCD anxiety- actually gives weight to the obsession and makes it more powerful. Instead, therapy for OCD is focused on breaking the connection between the obsession and compulsion, or interfering at this point in the cycle:
That means that a big part of therapy is having an obsession, feeling anxious about it……and sitting with that feeling. One type of therapy which utilizes this technique is called Exposure and Response Prevention (ERP), which involves tackling compulsions in a gradated order to build confidence. Patients may have weekly "challenges" that they have to engage in as they start to break down that cycle. For children, treatment of OCD often involves educating the whole family unit, in order to have everyone on the same page, and to prevent other family members from inadvertently engaging in compulsions. In addition, psychiatric treatment is often indicated, as medications such as Selective Serotonin Reuptake Inhibitors (SSRIs) can help to "quiet down" the obsessions and make engaging in the challenges easier.
OCD is a challenging thing to overcome, but by no means impossible with the correct treatment. The treatment is simple in theory, though complicated in practice, which means that it requires a clinician who is familiar with what OCD feels like and how to stop that cycle in its tracks. It is a misunderstood disorder, but there are increasing resources dedicated to breaking down this stigma. Some of my favorites include:
@Obsessivelyeverafter, an psychologist-run Instagram account dedicated to educating others about OCD
The YouTube channel run by Natasha Daniels, an anxiety and OCD therapist. A lot of her videos provide practical solutions to help parents manage the OCD compulsions of their child: https://www.youtube.com/c/AnxiousToddlers78
Anything written by the experts at the International OCD Foundation: https://iocdf.org/about-ocd/ or The Child Mind Institute: https://childmind.org/topics/ocd-related-disorders/
If you have any additional questions about OCD, please feel free to reach out to us using the Contact Us button.